Low back pain is very common, and the majority of the patients get better with time. The ideal patient will get better with time and has no radiation below the knee, no history of trauma, no fever or chills or weight loss, no bladder or bowel dysfunction, no neurological deficits, and no pathological reflexes.
In order to optimize recovery, management of the patient should consist of early return to activity as tolerated, as the symptoms allow. You will give the patient reassurance with limited analgesia, early range of motion, and muscle relaxants. A healthy patient with an acute onset of non-traumatic low back pain, you do not need early diagnostic imaging before proceeding with the therapeutic treatment. Diagnostic imaging is not necessary unless the initial treatment is unsuccessful, and the symptoms are prolonged. X-rays may not be needed in the first six weeks unless there is a reason for it, such as red flags. In fact, the use of x-rays can lead to better patient satisfaction but doesn’t necessarily lead to better patient outcome. X-rays and MRIs may show changes in the intervertebral discs and may be associated with the patient’s pain, but these changes are also commonly seen in cross-sectional studies of asymptomatic people. There are a lot of false positive MRIs, and you need to correlate the MRI findings with the clinical findings. Don’t rely on the MRI alone! Just because you have MRI changes or disc protrusion, it does not mean that the patient needs surgery!
A nonspecific pain does not require surgery; therefore, it does not require further work-up. There are risk factors associated with low back pain that includes Poor physical fitness; Smoking; History of repetitive bending or stooping on the job and whole-body vibration exposure. If the patient has a simple low back pain, 50% of the patients resolve their pain in one week. Resolution of the acute back pain occurs in 90% of the patients within one month. If the patient has leg pain greater than back pain, then the patient has sciatica. Sciatica means nerve root irritation, probably due to a herniated disc.
Maisonneuve fracture involves fracture of the proximal fibula associated with an occult and unstable injury of the ankle. The problem in these patients occur when the ankle injury is presented without a fracture of the lateral malleolus, or the medial malleolus and the injury is mistakenly diagnosed as an ankle sprain and the proximal fibular fracture is missed. Examine the leg for tenderness in the proximal fibula to diagnose a proximal fibula fracture. The patient could be mistakenly treated for having an isolated proximal fibular fracture alone and the ankle injury is missed.
High index of suspicion is necessary to diagnose and treat this injury. Maisonneuve fracture equals syndesmotic injury. Syndesmotic Injury equals Syndesmotic Reduction and Fixation. If ankle x-rays show medial or posterior malleolus fracture, or a medial clear space widening with no fracture of the lateral malleolus, then you must obtain a long-leg films to assess possible proximal fibular fracture. Clinical examination of their entire leg for pain and tenderness in addition to long leg films of the entire leg that includes the ankle, and the knee is mandatory in case of the patient with approximate fibular fracture to exclude the presence of an additional ankle injury, or if the patient has an unexplained increase in the medial clear space of the ankle joint. You should be searching for the presence of a high fibular fracture. Look for signs of syndesmotic injury such as an unexplained increase in medial clear space or tibiofibular clear space is widened and it should be less than 5 millimeters.
So how do you explain this injury? It is explained by the presence of rotation force to the ankle with transmission of the force through the interosseous membrane, which exits through a proximal fibular fracture. Maisonneuve fracture occurs from external rotation of the foot, most often with pronation mechanism. This force has to go somewhere! If you don’t see a fracture of the fibula then do the squeeze test or the external rotation stress test (both will show syndesmotic). The injury can involve the deltoid ligament injury or medial malleolar fracture medially and a fibular fracture proximally. Additionally, the tibiofibular ligaments are also involved, which can be the anterior tibiofibular ligament, interosseous ligament, the posterior tibiofibular ligament or posterior malleolar fracture. This looks like a very unstable ankle injury that may not be very obvious at presentation and you have to look out for it.
So how do you treat an Maisonneuve Fracture? This treated by fixation of the tibiofibular syndesmotic injury (key of treatment) or syndesmotic screws. if you have a medial site injury and there is a tear of the deltoid ligament, leave it alone. if there’s a medial malleolus fracture you should fix that of the lateral side if there’s approximate fibular fracture leave it alone. If there is a medial malleolar fracture, it should be fixed. If there is a proximal fibular fracture on the lateral side, leave it alone. As for the Syndesmotic Injury, the fixation has to be stable and adequate. Because of the magnitude of the injury, the Maisonneuve fracture may require more syndesmotic screws than with a routine ankle fracture with syndesmotic injury. After the fixation you will give a short leg non-weight bearing splint for six to eight weeks. Here is a patient taste example: the proximal fibular fracture and you can see increase in the medial clear space and you can see that the syndesmosis is widened. You can see that in the posterior malleolar fracture the patient is fixed with syndesmotic screws.
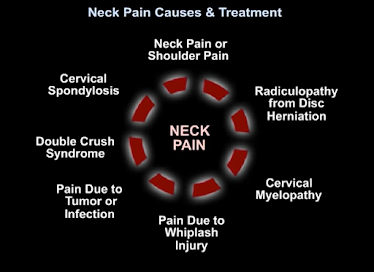
Neck pain is a common ailment of the American population, affecting 30 to 50% of adults annually. While there are numerous etiologies of neck pain, this is a brief review of the more common causes and modes of treatment.
Firstly, radiculopathy from disc herniation. In addition to neck pain, the patient will complain of arm pain that typically follows a myotomal pattern, and sensory symptoms (like burning and tingling) that follow a specific dermatome in the hand. There may also be motor weakness of the upper extremity. This is due to compression of a nerve root either by a disc herniation or by arthritis that narrows the foramen. A neurological exam assessing motor, sensory and reflex testing should be done to determine cervical spine disc herniation. Treatment should first be non-surgical with anti-inflammatory medication, isometric exercises, physical therapy, and muscle relaxants. An MRI should be ordered if symptoms do not improve after 6–12 weeks of conservative treatment. If there is an indication for surgery, it often involves decompression and fusion of the involved disc space. 26% of patients with cervical radiculopathy require surgery.
Secondly, neck pain may be due to cervical myelopathy. This is the most common cause of non-traumatic spinal cord dysfunction. It is due to direct compression of the spinal cord or surrounding blood vessels, and presents in a variety of ways clinically. Indications of cervical myelopathy are an unstable and wide-based gait, clumsiness of the hands, occipital headaches, and discomfort of the neck. The pain may not be severe, but insidious, gradual, and poorly characterized. An MRI may be ordered which will show compression of the spine. Due to the slow, stepwise deterioration in cervical myelopathy, each stage may be treated differently. There is conflicting evidence regarding the conservative versus surgical approach to treatment of cervical myelopathy. The goal for surgery is cord decompression with expansion of the spinal canal, restoration of cervical lordosis, and stabilisation if the risk of cervical kyphosis is high. The evidence suggests mild cervical myelopathy should be treated conservatively with careful observation, whereas surgical intervention should be employed for moderate to severe cases.
Thirdly, neck pain may be due to a whiplash injury. This is the most common traumatic cause of neck pain. Specifically, neck hyperreflexia and neck pain after a car collision from behind. Pain may refer to the head, shoulder, or arm. There are usually no neurological deficits. The patient will have a soft tissue injury and an x-ray will show cervical lordosis due to muscle spasm. Treatment for a whiplash injury is aggressive physical therapy and mobilization.
Cervical spondylosis may also cause neck pain. This is arthritis of the spine. It is a natural degenerative process of cervical spine which will be shown on X-Ray. Degenerative changes start in the intervertebral discs with osteophyte formation and involvement of soft tissue structures. It is important to note many people over 30 years of age display similar abnormalities on imaging of the cervical spine and it may be difficult to delineate normal aging and disease. Cervical spondylosis can be diagnosed clinically based on characteristic exacerbation by neck movement. Although pain is focused in the cervical area, it is also referred to a wide area. Cervical spondylosis should be managed medically and surgery should only be done if there is instability or neurological deficit. In fact, there is evidence that suggests various exercise regiments may be more effective than usual medicinal care (analgesics, muscle relaxants) or stress management.
While there are various pathologies to include in the differential of neck pain, typically, patients with neck pain will have no injury. Pain will be in the posterior neck, tender to palpation with no radiation to the arm, no neurological deficits, and an X-Ray will show mild arthritis. Often, patients will be prescribed anti-inflammatory medication and referred to physical therapy.
References
1. Goode AP, Freburger J, Carey T. Prevalence, practice patterns, and evidence for chronic neck pain. Arthritis Care Res (Hoboken). 2010 Nov;62(11):1594–601. doi: 10.1002/acr.20270. Epub 2010 Jun 2. PMID: 20521306; PMCID: PMC2974793.
3. Wong JJ, Côté P, Quesnele JJ, Stern PJ, Mior SA. The course and prognostic factors of symptomatic cervical disc herniation with radiculopathy: a systematic review of the literature. Spine J. 2014; 14(8):1781–9.
4. Bakhsheshian J, Mehta VA, Liu JC. Current Diagnosis and Management of Cervical Spondylotic Myelopathy. Global Spine J. 2017 Sep;7(6):572–586. doi: 10.1177/2192568217699208. Epub 2017 May 31. PMID: 28894688; PMCID: PMC5582708.
5. MacDermid JC, Walton DM, Bobos P, Lomotan M, Carlesso L. A Qualitative Description of Chronic Neck Pain has Implications for Outcome Assessment and Classification. Open Orthop J. 2016 Dec 30;10:746–756. doi: 10.2174/1874325001610010746. PMID: 28217199; PMCID: PMC5301418.
6. Binder AI. Cervical spondylosis and neck pain. BMJ. 2007 Mar 10;334(7592):527–31. doi: 10.1136/bmj.39127.608299.80. PMID: 17347239; PMCID: PMC1819511.
Sacroiliac Joint pain can often be inappropriately treated or mistaken as lower back pain. There are several conditions that simulate sacroiliac joint pain.
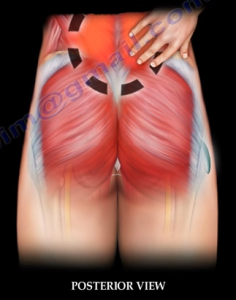
1. Myofascial Pain
This is a chronic pain caused by multiple trigger points and fascial constrictions. This particular condition involves the muscles and fascial areas of the back. The patient may feel knots or hardening of the muscle with weakness and tenderness. Myofascial pain syndrome and fibromyalgia may present the same clinical picture but, they are different problems. The site location is close to the SI joint and can be confused with SI joint pain.
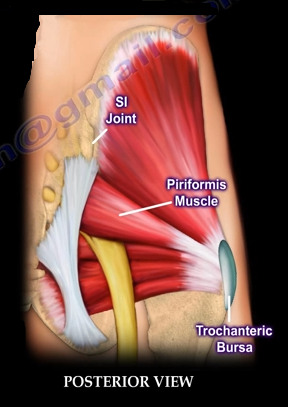
2. Trochanteric Bursitis
Inflammation of the greater trochanter bursa. This condition causes tenderness and pain in the hip. Trochanteric bursitis occurs in middle aged women. The area of pain may overlap with the SI joint area of pain and can radiate close to the sacroiliac joint. The pain from this condition is sometimes severe and associated with iliotibial band syndrome. Trochanteric Bursitis is occasionally overlooked. This condition may present with arthritis of the hip and low back pain and other conditions.
3. Piriformis Syndrome
This condition occurs when the sciatic nerve is compressed by the piriformis muscle in the buttocks. Piriformis Syndrome may be associated with lower lumbar radiculopathy similar to spine pathology. It occasionally develops due to blunt trauma to the buttocks. Localized buttocks pain will increase with sitting or driving. Tenderness is commonly found in the sciatic notch.
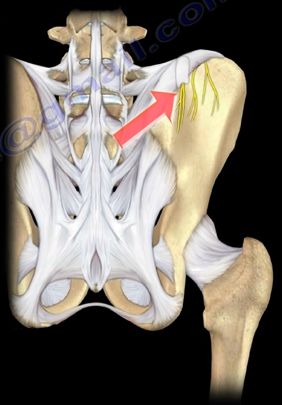
4. Cluneal Nerve Entrapment
The superior cluneal nerve has three branches. The medial branch of this nerve is confined within a tunnel which may cause impingement of the nerve producing pain close to the SI joint.
5. Lumbosacral Disc Herniation or Bulge
The disc may move out of place (herniate) or break open (rupture) from injury or strain. Disc herniation of the lumbosacral region could involve the nerve roots, creating lower back pain. The pain is usually found in the midline and can go down the leg.
6. Lumbosacral Facet Syndrome
The facet provides stability for the spine and contain a joint. This joint may be affected by inflammations or degeneration which causes pain that can be mistaken for SI joint pain.
7. Lumbar Radiculopathy
Lumbar Radiculopathy is a major source of back pain. This condition occurs from inflammation, irritation, or impingement of the nerve root. It is commonly confused for SI joint pain.

 in the hip. Trochanteric bursitis occurs in middle aged women. The area of pain may overlap with the SI joint area of pain and can radiate close to the sacroiliac joint. The pain from this condition is sometimes severe and associated with iliotibial band syndrome. Trochanteric Bursitis is occasionally overlooked. This condition may present with arthritis of the hip and low back pain and other conditions.
in the hip. Trochanteric bursitis occurs in middle aged women. The area of pain may overlap with the SI joint area of pain and can radiate close to the sacroiliac joint. The pain from this condition is sometimes severe and associated with iliotibial band syndrome. Trochanteric Bursitis is occasionally overlooked. This condition may present with arthritis of the hip and low back pain and other conditions.
 The superior cluneal nerve has three branches. The medial branch of this nerve is confined within a tunnel which may cause impingement of the nerve producing pain close to the SI joint.
The superior cluneal nerve has three branches. The medial branch of this nerve is confined within a tunnel which may cause impingement of the nerve producing pain close to the SI joint.
 The facet provides stability for the spine and contain a joint. This joint may be affected by inflammations or degeneration which causes pain that can be mistaken for SI joint pain.
The facet provides stability for the spine and contain a joint. This joint may be affected by inflammations or degeneration which causes pain that can be mistaken for SI joint pain.
