Extension contracture of the knee can result from different causes, but it usually occurs from trauma. The patient is unable to bend the knee to a functional level.
Trauma will cause adhesions inside the knee, fibrosis, and shortening of the knee ligaments.
There will also be adhesions and shortening of the quadriceps muscles.
Treatment
Treatment will usually begin with therapy. The first surgical option will include an arthroscopy and the release of any adhesions. The second surgical option that may be considered as a quadricepsplasty (Thompson or Judet) or a combination of treatments.
An example of a combination treatment plan would be a modified Judet quadricepsplasty with the release of the quadriceps muscle from the femur and a release of the adhesions that are located inside the knee.
After surgery the surgeon can usually achieve 90° plus flexion.
Osteonecrosis or avascular necrosis of the hip is death of a segment of bone in the femoral head due to disruption of the blood supply. The etiology of this condition is not fully understood. There are several risk factors associated with osteonecrosis of the hip.
The condition is bilateral in about 80% of the patients. Check the other hip even if it is asymptomatic.
Early diagnosis is important. In early stages of osteonecrosis, a femoral head preserving procedure may be done. In late stages of osteonecrosis, the femoral head collapses and cannot be saved. The femoral head may need to be replaced.
Obtain AP frog leg lateral views of the hip. The frog leg lateral view will show the crescent sign. MRI is the study of choice especially when the patient has persistent hip pain, radiographs are negative and the diagnosis of osteonecrosis is suspected.
The Ficat classification is a commonly used system to stage osteonecrosis of the hip.
Stage I: normal appearing X-ray. MRI will detect the lesion (changes in the marrow).
Stage II: sclerosis and cyst formation
Stage III: subchondral fracture. Crescent sign and flattening of the femoral head.
Stage IV: advanced lesions with arthritis, osteophyte formation and loss of the joint space.
Treatment
For early stages of osteonecrosis of the hip, initial trial of non surgical treatment is usually done. Surgery may be needed if non surgical methods are not successful.
Non-operative treatment includes:
Bisphosphonates: may also be used before the femoral head collapses. Still experimental.
Traditional surgical treatment: when the lesion is small, a head preserving procedure can be done.
Core decompression for stages I and II: can make a single large hole or multiple holes in the femoral head. It decompresses the head and stimulates a healing response. The lesion is anteriorly and superiorly.
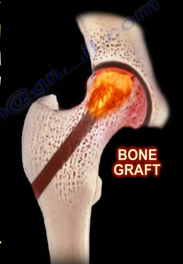
Core decompression with bone graft: debride the necrotic area and place the bone graft. Some lace this much bone graft.
Traditional fibular graft: is done in younger patients.
Complications:
Donor site pain and leg dysfunction
Tibial stress fracture form side the graft is taken.
Total hip arthroplasty (cementless cup and stem) or total hip resurfacing. Resurfacing is not commonly used.
Total hip replacement (predictable): is considered to be the traditional procedure for advanced stages of osteonecrosis of the hip.
Total hip resurfacing (controversial): need adequate bone stock to support the femoral component. The result is not as good when compared with a patient with osteoarthritis (older group).
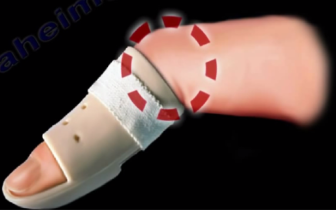
Fractures to the fingers and hands are common. Mallet finger is a deformity caused from a blow to the finger at the DIP joint. Patient is unable to straighten the DIP due to avulsion injury.
Most often mallet finger injuries can be treated without surgery. Treatment is given by applying a splint to immobilize the fingertip in extension. Movement should be allowed in the PIP joint. Surgery may be necessary if more than 50% of the joint is involved or there is subluxation of the joint to restore the function of the extensor tendon.
Middle and proximal phalangeal fractures:
The normal relaxed cascade of the hand should form a straight alignment of the fingers. When holding a relaxed cascade, the fingers should normally point towards the region of the scaphoid. Malrotation of the finger will cause the affected finger to deviate from its normal rotational direction.
Treatment:
If there is no rotational deformity, the finger is treated by buddy taping the injured finger to the adjacent normal finger for 2-3 weeks. If rotational deformity is present, a digital block is given and the fracture is reduced in a volar splint. The MCP is held in 70 degrees of flexion for proximal phalanx fractures for 2-3 weeks. The splint holds the DIP and PIP in 0 degrees extension in middle phalanx fractures. Then buddy tape for additional 2 weeks.
Metacarpal fractures:
The wrist should be immobilized in 20 degrees extension and the MCP in 60-70 degrees of flexion.
The fingers should be kept free in order to check for rotation. Finger fractures means stiffness of the fingers.
Indication for surgery:
Rotational deformity
Open fracture
Multiple unstable fractures
Significant angulation or deformity.
Articular displacement
Metacarpal shortening especially with the middle and index fingers.
If the fracture is displaced or unstable, closed reduction and K-wire is an option for fixation.
Plating is another option for fixation however it is rare.
In phalanx fractures treated by ORIF, adhesions of the extensor tendon may occur. Patient may have decreased range of motion of the PIP which is called extrinsic tightness.
The patient will have greater passive PIP flexion with MP extension compared to when MP is flexed.
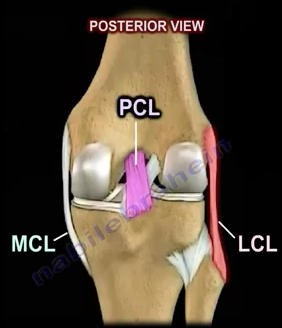
The dial test is performed to diagnose posterolateral instability due to posterolateral corner injury with or without a PCL injury.
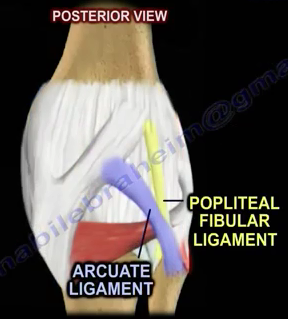
Isolated injuries of the posterolateral corner are rare and often cause instability and varus thrust. By performing the Dial test, you can detect whether there is an isolated or combined injury of the posterolateral corner of the knee. Usually this injury is combined with a cruciate ligament injury (more with the PCL than the ACL).
Failure to identify the posterolateral corner injury combined with injury to the ACL will lead to failure of ACL reconstruction. Therefore, it is important to properly diagnose this injury! This means that the posterolateral corner is injured and the posterior cruciate ligament is not injured. MRI is the diagnostic study of choice for this injury.
How do you perform the Dial test?
The dial test is performed with the patient in the supine or prone position with both knees in 30° and 90° of flexion. It is preferable to perform the test in the prone position. Support the thigh in position if you are going to perform the test in the supine position. An external rotational force is then applied to both feet. The amount of external rotation to both lower extremity is measured at both ankles. Testing of the injured extremity in 30° of flexion is done to determine injury to the posterolateral corner. Flexion at the 90° angle will test the posterior cruciate ligament (PCL) for injury. More than 10° of external rotation indicates a significant injury. More than 10° of external rotation asymmetry at 30° and 90° is consistent with PLC and PCL injury.
Imaging
Proximal medial open wedge tibial osteotomy should be done for primary varus of the knee before reconstruction of the PLC, otherwise reconstruction will fail. Obtain a long leg standing x-ray before surgery to check if the varus is primary or secondary.