A physeal injury in the distal femur in the neonate is rare. In general, traumatic neonatal physeal fracture usually occurs in the distal humerus and rarely occurs in the distal femur. The condition usually occurs due to birth trauma and usually results due to physeal separation which results in epiphyseal separation. The thigh will be swollen and there may be hypomobility of the extremity. The neonate will be fussy or irritated with significant swelling in the thigh. The condition is under diagnosed. The epiphysis is usually present at birth on x-rays. This condition can become complicated if the epiphysis is not completely ossified at birth or if the child is born prematurely. In this situation, the x-ray interpretation may be difficult. An MRI will be really helpful if the doctor is uncertain of the diagnosis. X-rays should be taken at the child at birth. The physician should look at the lateral x-ray and find the epiphysis is present and ossified at birth with varying degrees (may not be clear). Each epiphysis will line up with its corresponding bone. Epiphysis of the distal femur should line up with the femoral shaft. Epiphysis of the proximal tibia should line up with the tibial shaft. If the two epiphysis separate from each other, then this is a congenital dislocation of the knee. This can be a spectrum of injury that varies from hyperextension to subluxation, to frank dislocation. If the epiphysis is separated from its corresponding bone, for example, the epiphysis of the distal femur is separated from the shaft of the femur, then this is a physeal injury. Because the distal femur is mostly cartilaginous, you don’t see bone shifting, you see a little hint of the separation of the physis by seeing that the small ossified epiphysis is not in its normal position that corresponds with the axis of the bone. You need to know the difference between physeal injury and congenital dislocation of the knee. Accurate, gentle closed reduction with follow-up x-rays to confirm the reduction and to detect any early bony bridging.
There are three different types of osteonecrosis of the knee. There is Spontaneous Osteonecrosis of the Knee, Post Arthroscopic Osteonecrosis of the knee, and Secondary Osteonecrosis of the knee. Osteonecrosis is further classified by severity using Ficat Stages of Knee Osteonecrosis. In Stage I, the x-ray appears normal. Stage II, Sclerosis of the condyle is present. In Stage III, the crescent sign is found as well as a subchondral fracture. Stage IV, there is a collapse of subchondral bone.
Spontaneous Osteonecrosis of the Knee typically occurs in females older than 55. Usually one joint and one compartment is affected (medial femoral compartment). No etiology is known. Symptoms typically consist of a sudden onset of severe pain with decreased range of motion as well as swelling in the knee. X-rays will probably appear to be normal. An MRI is helpful, the provider may find a crescent shaped lesion. This condition can cause arthritis. If severe knee pain is present in a middle aged or elderly female patient, and the x-ray is negative, the provider should order an MRI to rule out osteonecrosis of the knee. Treatment consists of protected weightbearing as well as therapy and NSAIDs. An arthroplasty may be required when conservative treatment fails. A unicompartmental knee arthroplasty will be performed for small lesions. A total knee arthroplasty will be completed for large lesions or collapse.
Post Arthroscopy Osteonecrosis of the Knee most commonly occurs in middle aged women after a knee arthroplasty. Secondary Osteonecrosis of the knee is common in women under 55 years of age and has associated risk factors. This condition involves more than one compartment or the metaphysis of the knee. Secondary Osteonecrosis occurs bilaterally in 80% of cases and multifocal lesions may be seen. There is a cause for Secondary Osteonecrosis of the knee, which is why it can be bilateral, multiple, and everywhere. Risk factors include:
Alcohol use
Sickle cell disease
Steroid use
Trauma
HIV medications
Gaucher Disease
These patients should be screened for other joint involvement. The lesion is a subcondylar insufficiency fracture and the patient will have severe pain with weight bearing either standing or sitting. An x-ray may show a wedge-shaped lesion and MRI is the better study. A differential diagnosis is Osteochondral Dissecans, which is located in the lateral aspect of the medial femoral condyle in younger patients. Other differentials include: Occult trauma, bone bruise and overuse, as well as transient osteoporosis which is found more in middle-aged men and usually in the hip rather than the knee. Treatment consists of NSAIDs, a decrease in activity and weightbearing, and physical therapy. A scope surgery may be necessary to remove loose fragments or core decompression for lesions not extending to the joint. An Osteocondylar allograft may be performed for large, painful lesions in younger patients. A total knee replacement may be done for larger lesions, for collapse, or if multiple compartments are involved. Conservative treatment is not as successful with secondary avascular necrosis. Without surgery, secondary AVN will advance to osteoarthritis. Bisphosphonates have no effect on knee osteonecrosis.
Supracondylar fractures constitute approximately 50% of all elbow fractures. The supracondylar region is thin and weak and thus can fracture easily. These fractures are classified into two different types: extension and flexion.
Extension type fractures are the most common type, occurring approximately 95% of the time. Extension fractures typically occur due to falling onto an outstretched hand. With extension fractures, the distal fragment of the humerus displaces posteriorly. Anterior interosseous neurapraxia is the most common nerve palsy occurring with supracondylar fractures. Injury to the anterior interosseous nerve will lead to weakness of the flexor digitorum profundus muscle to the index finger and the flexor pollicis longus muscle. The patient will not be able to make an “OK” sign or bend the tip of his index finger. Radial nerve neurapraxia is the second most common palsy and is evident by weakness in wrist and finger extension.
The second type of fractures, flexion type fractures are rare and occurs due to falling directly on a flexed elbow. In flexion type fractures, the distal fragment is displaced anteriorly. This type of fracture may be accompanied with ulnar nerve neurapraxia. Injury to the ulnar nerve will lead to a loss of sensation along the little finger. Later on, the patient may also have weakness of the intrinsic hand muscles and clawing.
Gartland Classification System
The Gartland Classification System provides physicians with a way to categorize supracondylar humerus fractures. There are four classifications and are as follows: Type I fractures are nondisplaced fractures; Type II are angulated with an intact posterior cortex; Type III are completely displaced; and Type IV has complete periosteal disruption with instability in both flexion and extension.
Radiology
Plain AP and lateral x-rays should be obtained. A posterior fat pad sign seen on a lateral view x-ray should increase your suspicion of an occult fracture around the elbow. On a lateral view x-ray, the anterior humeral line is drawn along the anterior border of the distal humerus. Normally, the anterior humeral line should run through the middle third of the capitellum. In extension type fractures, the capitellum will be displaced posteriorly, relative to the anterior humeral line.
The Baumann’s Angle is formed by a line perpendicular to the axis of the humerus and a line going through the physis of the capitellum. Normally, the Baumann’s angle should measure at least 11° (variable).
Physical Examination
It is important to assess the neurovascular structures. The anterior interosseous nerve is assessed by asking the patient to do the “OK” sign with their hand. The radial nerve is assessed by asking the patient to extend their wrist and fingers. Ulnar nerve damage is usually indicated by the loss of sensation along the little finger; however, later on the patient may have weakness of the intrinsic hand muscles and clawing.
Treatment
Nonoperative treatment is usually indicated for type I fractures. This treatment usually consists of splinting or casting the elbow for a duration of 3-4 weeks. It is very important to remember not to flex the elbow in the splint or cast beyond 90° in order to avoid vascular compromise and compartment syndrome.
Operative treatment is usually indicated for Types II and III, and are usually treated by a closed reduction and percutaneous pinning. During reduction, pronation of the forearm during elbow flexion helps to correct a varus deformity. After reduction, the surgeon will want to check for a gap in the fracture, as the neurovascular bundle may be trapped there. The surgeon will need to free the brachialis muscle from the fracture site if it is interpositioned there. Fixation is usually achieved with 2-3 divergent lateral pins, depending on stability. Medial pins may also be added depending on stability; however, the surgeon will need to be aware of the ulnar nerve when placing the medial pin.
Open reductions are only performed when closed techniques are unable to achieve the appropriate reduction of the fracture. The surgeon will want to avoid posterior dissection in order to preserve the vascularity of the fractured segment. Fracture reduction and fixation should be done emergently in cases of vascular compromise.
Complications
Neurapraxia is a common complication of supracondylar fractures and usually resolves on its own—thus, treatment is observation only. A cubitus varus deformity may occur due to a malunion of the fracture. This only presents as a cosmetic problem since it does not affect the function of the arm or elbow. Additionally, this deformity can be corrected later on by a supracondylar valgus osteotomy. Vascular problems, such as compartment syndrome, may also occur. Volkmann’s ischemic contracture may occur due to a compression of the brachial artery with then patient is placed in a cast with the arm in hyperflexion (more than 90°).
Important Scenerios
A patient may present with a Displaced Type III fracture and a pulseless hand. He may have adequate circulation—which is evident by the normal temperature and color of the hand—or he may have inadequate circulation—indicated by a cold blue hand. In both cases, an urgent closed reduction and percutaneous pinning is required. Once this has been performed and the circulation is adequate, the surgeon can observe the patient and place them in a splint that is at a 45° angle. However, if the patient continues to have inadequate circulation after the closed reduction, then the patient will require a vascular exploration and repair.
X-rays ionize human tissue and deposit energy that can cause harmful changes within the body (break the DNA chain). Additionally, there is a cancer risk from exposure to x-rays. The dose of radiation is cumulative. X-rays are considered carcinogenic. The government is attempting to minimize the use of unnecessary CT scans and x-rays to prevent unnecessary exposure to radiation. It is important for doctors to pay close attention to the risks involved with the use of x-rays. The cancer risk associated with radiation exposure is documented in cases of atomic bomb survivors.
The risk for medical uses is controversial and usually played down by physicians. Radiation at a high level is carcinogenic but, the level of radiation from x-ray exposure is low. The effects of low level radiation is not known.
What is the safe radiation level?
The safe level of radiation is not known.
It is known that CT scans, fluoroscopy, mammography, and x-rays expose the public to high levels of radiation, especially in young females. The risk of exposure should balance the medical benefits.
Optimize radiation doses by only exposing the patient to enough radiation to get a clear image. There is a growing concern about the risk associated with giving a patient large doses of radiation. The use of CT scans has increased recently in adults and children, possibly exposing the patient to an unnecessarily high dose of radiation. A CT scan is often the method used to diagnose cancer, diseases, and fractures, exposing the patient to a much larger dose of radiation than x-rays. Radiation from a CT scan of the pelvis equals the same amount as 100 chest x-rays. Children are ten times more sensitive to radiation than adults. 3-4 million children receive CT scans and about 1,500 of them will develop cancer two decades later. Additionally, children should not be given an adult dose of radiation.
Radiation Dose Limits
A CT scan of the pelvis has the highest level of exposure to the skin, marrow, and gonads. A mini fluoroscopy C-arm should be used whenever possible. Fluoroscopy emits a lot of radiation. The closer the extremity is to the radiation source, the higher the dose of radiation the patient receives. When the distance from the beam increases, the dose of radiation is less. Attempt to decrease exposure time. Radiation intensity follows the inverse square law. It is all about distance!
If the intensity of radiation at 1 meter from the source is 100mR/hr, then the intensity of radiation at 2 meters from the source is ¼ or 25mR/hr in the same unit area. At 3 meters from the source, the intensity of radiation is 1/9 the original or 11.1mR/hr.
Units of Radiation
Roentgen
Unit of radiation exposure in the air
Rad
Energy absorbed per gram of tissue
Rem
Biological effect of a rad
There is less exposure to the physician when imaging a smaller body part. Larger body parts create an increased exposure to the physician when imaging a patient with the C-arm. It is important to not be in the direct path of the radiation beam.
Methods of protection include: monitoring, shielding, and position. A dosimeter badge records how much radiation you have received; however, it does NOT protect you from exposure to radiation. Lead gowns and aprons work to stop exposure to fluoroscopic radiation. Lead aprons attenuate scattered radiation by about 95%. Rapidly dividing cells are most sensitive to radiation exposure and include: sperm, lymphocytes, and cells inside the small intestine and stomach.
Radiation damage seldom appears at the time or irradiation. The first effects of radiation damage is usually seen as a drop in the white blood cell count. The first external sign of damage is usually a skin burn. Studies suggest that people who use fluoroscopy extensively have a higher rate of cataracts.
Early effects of radiation exposure include:
Death
Hematologic depression
Chromosome aberration
Skin erythema
Epilation
My recommendations:
A CT scan examination is usually done without justification by most insurances. In my opinion, 1/3 of CT scan studies that are given could be avoided; they are an added cancer risk with no benefit. The CT scan study should be justified. There is no close oversight or uniform standard in place to eliminate radiation exposure, and this is something that should be taken seriously.
Patient education is important. The patient should ask if the study is necessary and what is the lowest dose possible that can be given without compromising the study. Additionally, there should be a universal x-ray bank where patient’s x-rays can be accessed by any medical facility. This would eliminate the unnecessary repeating of x-rays.
In summary, the bone marrow, breast tissue, gonads, and lymphatic tissue are susceptible to radiation induced tumors. It is important to shield the gonads from exposure. Always wear protective equipment such as lead aprons and monitor your radiation exposure with the dosimeter badge.

 shaft. Epiphysis of the proximal tibia should line up with the tibial shaft. If the two epiphysis separate from each other, then this is a congenital dislocation of the knee. This can be a spectrum of injury that varies from hyperextension to subluxation, to frank dislocation. If the epiphysis is separated from its corresponding bone, for example, the epiphysis of the distal femur is separated from the shaft of the femur, then this is a physeal injury. Because the distal femur is mostly cartilaginous, you don’t see bone shifting, you see a little hint of the separation of the physis by seeing that the small ossified epiphysis is not in its normal position that corresponds with the axis of the bone. You need to know the difference between physeal injury and congenital dislocation of the knee. Accurate, gentle closed reduction with follow-up x-rays to confirm the reduction and to detect any early bony bridging.
shaft. Epiphysis of the proximal tibia should line up with the tibial shaft. If the two epiphysis separate from each other, then this is a congenital dislocation of the knee. This can be a spectrum of injury that varies from hyperextension to subluxation, to frank dislocation. If the epiphysis is separated from its corresponding bone, for example, the epiphysis of the distal femur is separated from the shaft of the femur, then this is a physeal injury. Because the distal femur is mostly cartilaginous, you don’t see bone shifting, you see a little hint of the separation of the physis by seeing that the small ossified epiphysis is not in its normal position that corresponds with the axis of the bone. You need to know the difference between physeal injury and congenital dislocation of the knee. Accurate, gentle closed reduction with follow-up x-rays to confirm the reduction and to detect any early bony bridging. 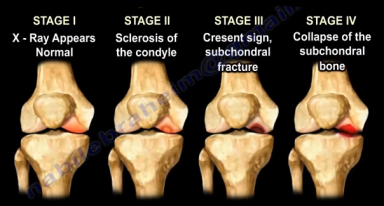 Spontaneous Osteonecrosis of the Knee typically occurs in females older than 55. Usually one joint and one compartment is affected (medial femoral compartment). No etiology is known. Symptoms typically consist of a sudden onset of severe pain with decreased range of motion as well as swelling in the knee. X-rays will probably appear to be normal. An MRI is helpful, the provider may find a crescent shaped lesion. This condition
Spontaneous Osteonecrosis of the Knee typically occurs in females older than 55. Usually one joint and one compartment is affected (medial femoral compartment). No etiology is known. Symptoms typically consist of a sudden onset of severe pain with decreased range of motion as well as swelling in the knee. X-rays will probably appear to be normal. An MRI is helpful, the provider may find a crescent shaped lesion. This condition can cause arthritis. If severe knee pain is present in a middle aged or elderly female patient, and the x-ray is negative, the provider should order an MRI to rule out osteonecrosis of the knee. Treatment consists of protected weightbearing as well as therapy and NSAIDs. An arthroplasty may be required when conservative treatment fails. A unicompartmental knee arthroplasty will be performed for small lesions. A total knee arthroplasty will be completed for large lesions or collapse.
can cause arthritis. If severe knee pain is present in a middle aged or elderly female patient, and the x-ray is negative, the provider should order an MRI to rule out osteonecrosis of the knee. Treatment consists of protected weightbearing as well as therapy and NSAIDs. An arthroplasty may be required when conservative treatment fails. A unicompartmental knee arthroplasty will be performed for small lesions. A total knee arthroplasty will be completed for large lesions or collapse. women after a knee arthroplasty. Secondary Osteonecrosis of the knee is common in women under 55 years of age and has associated risk factors. This condition involves more than one compartment or the metaphysis of the knee. Secondary Osteonecrosis occurs bilaterally in 80% of cases and multifocal lesions may be seen. There is a cause for Secondary Osteonecrosis of the knee, which is why it can be bilateral, multiple, and everywhere. Risk factors include:
women after a knee arthroplasty. Secondary Osteonecrosis of the knee is common in women under 55 years of age and has associated risk factors. This condition involves more than one compartment or the metaphysis of the knee. Secondary Osteonecrosis occurs bilaterally in 80% of cases and multifocal lesions may be seen. There is a cause for Secondary Osteonecrosis of the knee, which is why it can be bilateral, multiple, and everywhere. Risk factors include: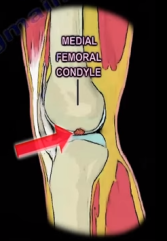
 Extension type fractures are the most common type, occurring approximately 95% of the time. Extension fractures typically occur due to falling onto an outstretched hand. With extension fractures, the distal fragment of the humerus displaces posteriorly. Anterior interosseous neurapraxia is the most common nerve palsy
Extension type fractures are the most common type, occurring approximately 95% of the time. Extension fractures typically occur due to falling onto an outstretched hand. With extension fractures, the distal fragment of the humerus displaces posteriorly. Anterior interosseous neurapraxia is the most common nerve palsy occurring with supracondylar fractures. Injury to the anterior interosseous nerve will lead to weakness of the flexor digitorum profundus muscle to the index finger and the flexor pollicis longus muscle. The patient will not be able to make an “OK” sign or bend the tip of his index finger. Radial nerve neurapraxia is the second most common palsy and is evident by weakness in wrist and finger extension.
occurring with supracondylar fractures. Injury to the anterior interosseous nerve will lead to weakness of the flexor digitorum profundus muscle to the index finger and the flexor pollicis longus muscle. The patient will not be able to make an “OK” sign or bend the tip of his index finger. Radial nerve neurapraxia is the second most common palsy and is evident by weakness in wrist and finger extension. directly on a flexed elbow. In flexion type fractures, the distal fragment is displaced anteriorly. This type of fracture may be accompanied with ulnar nerve neurapraxia. Injury to the ulnar nerve will lead to a loss of sensation along the little finger. Later on, the patient may also have weakness of the intrinsic hand muscles and clawing.
directly on a flexed elbow. In flexion type fractures, the distal fragment is displaced anteriorly. This type of fracture may be accompanied with ulnar nerve neurapraxia. Injury to the ulnar nerve will lead to a loss of sensation along the little finger. Later on, the patient may also have weakness of the intrinsic hand muscles and clawing.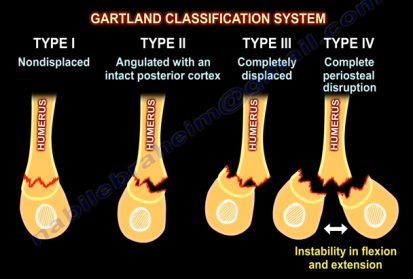 The Gartland Classification System provides physicians with a way to categorize supracondylar humerus fractures. There are four classifications and are as follows: Type I fractures are nondisplaced fractures; Type II are angulated with an intact posterior cortex; Type III are completely displaced; and Type IV has complete periosteal disruption with instability in both flexion and extension.
The Gartland Classification System provides physicians with a way to categorize supracondylar humerus fractures. There are four classifications and are as follows: Type I fractures are nondisplaced fractures; Type II are angulated with an intact posterior cortex; Type III are completely displaced; and Type IV has complete periosteal disruption with instability in both flexion and extension.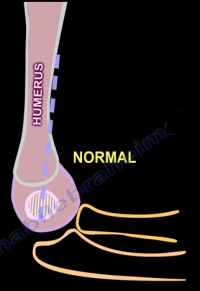 lateral view x-ray should increase your suspicion of an occult fracture around the elbow. On a lateral view x-ray, the anterior humeral line is drawn along the anterior border of the distal humerus. Normally, the anterior humeral line should run through the middle third of the capitellum. In extension type fractures, the capitellum will be displaced posteriorly, relative to the anterior humeral line.
lateral view x-ray should increase your suspicion of an occult fracture around the elbow. On a lateral view x-ray, the anterior humeral line is drawn along the anterior border of the distal humerus. Normally, the anterior humeral line should run through the middle third of the capitellum. In extension type fractures, the capitellum will be displaced posteriorly, relative to the anterior humeral line. Treatment
Treatment Operative treatment is usually indicated for Types II and III, and are usually treated by a closed reduction and percutaneous pinning. During reduction, pronation of the forearm during elbow flexion helps to correct a varus deformity. After reduction, the surgeon will want to check for a gap in the fracture, as the neurovascular bundle may be trapped there. The surgeon will need to free the brachialis muscle from the fracture site if it is interpositioned there. Fixation is usually achieved with 2-3
Operative treatment is usually indicated for Types II and III, and are usually treated by a closed reduction and percutaneous pinning. During reduction, pronation of the forearm during elbow flexion helps to correct a varus deformity. After reduction, the surgeon will want to check for a gap in the fracture, as the neurovascular bundle may be trapped there. The surgeon will need to free the brachialis muscle from the fracture site if it is interpositioned there. Fixation is usually achieved with 2-3  divergent lateral pins, depending on stability. Medial pins may also be added depending on stability; however, the surgeon will need to be aware of the ulnar nerve when placing the medial pin.
divergent lateral pins, depending on stability. Medial pins may also be added depending on stability; however, the surgeon will need to be aware of the ulnar nerve when placing the medial pin. deformity can be corrected later on by a supracondylar valgus osteotomy. Vascular problems, such as compartment syndrome, may also occur. Volkmann’s ischemic contracture may occur due to a compression of the brachial artery with then patient is placed in a cast with the arm in hyperflexion (more than 90°).
deformity can be corrected later on by a supracondylar valgus osteotomy. Vascular problems, such as compartment syndrome, may also occur. Volkmann’s ischemic contracture may occur due to a compression of the brachial artery with then patient is placed in a cast with the arm in hyperflexion (more than 90°). The risk for medical uses is controversial and usually played down by physicians. Radiation at a high level is carcinogenic but, the level of radiation from x-ray exposure is low. The effects of low level radiation is not known.
The risk for medical uses is controversial and usually played down by physicians. Radiation at a high level is carcinogenic but, the level of radiation from x-ray exposure is low. The effects of low level radiation is not known. It is known that CT scans, fluoroscopy, mammography, and x-rays expose the public to high levels of radiation, especially in young females. The risk of exposure should balance the medical benefits.
It is known that CT scans, fluoroscopy, mammography, and x-rays expose the public to high levels of radiation, especially in young females. The risk of exposure should balance the medical benefits. A CT scan of the pelvis has the highest level of exposure to the skin, marrow, and gonads. A mini fluoroscopy C-arm should be used whenever possible. Fluoroscopy emits a lot of radiation. The closer the extremity is to the radiation source, the higher the dose of radiation the patient receives. When the distance from the beam increases, the dose of radiation is less. Attempt to decrease exposure time. Radiation intensity follows the inverse square law. It is all about distance!
A CT scan of the pelvis has the highest level of exposure to the skin, marrow, and gonads. A mini fluoroscopy C-arm should be used whenever possible. Fluoroscopy emits a lot of radiation. The closer the extremity is to the radiation source, the higher the dose of radiation the patient receives. When the distance from the beam increases, the dose of radiation is less. Attempt to decrease exposure time. Radiation intensity follows the inverse square law. It is all about distance! Units of Radiation
Units of Radiation Methods of protection include: monitoring, shielding, and position. A dosimeter badge records how much radiation you have received; however, it does NOT protect you from exposure to radiation. Lead gowns and aprons work to stop exposure to fluoroscopic radiation. Lead aprons attenuate scattered radiation by about 95%. Rapidly dividing cells are most sensitive to radiation exposure and include: sperm, lymphocytes, and cells inside the small intestine and stomach.
Methods of protection include: monitoring, shielding, and position. A dosimeter badge records how much radiation you have received; however, it does NOT protect you from exposure to radiation. Lead gowns and aprons work to stop exposure to fluoroscopic radiation. Lead aprons attenuate scattered radiation by about 95%. Rapidly dividing cells are most sensitive to radiation exposure and include: sperm, lymphocytes, and cells inside the small intestine and stomach. Patient education is important. The patient should ask if the study is necessary and what is the lowest dose possible that can be given without compromising the study. Additionally, there should be a universal x-ray bank where patient’s x-rays can be accessed by any medical facility. This would eliminate the unnecessary repeating of x-rays.
Patient education is important. The patient should ask if the study is necessary and what is the lowest dose possible that can be given without compromising the study. Additionally, there should be a universal x-ray bank where patient’s x-rays can be accessed by any medical facility. This would eliminate the unnecessary repeating of x-rays.